If you are interested in products and services related to the research phase in this field, please contact for further inquiries.
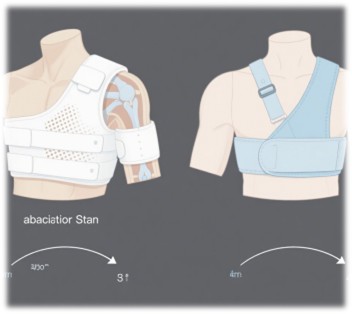
Rotator cuff repair is a common surgical procedure aimed at addressing one of the most prevalent shoulder disorders among older adults. Advances in arthroscopic techniques have revolutionized the approach to rotator cuff repair, offering less invasive and more effective solutions compared to traditional open surgeries. However, the optimal postoperative immobilization strategy remains a contentious issue within the medical community. This article delves into the comparative analysis of two widely used immobilization methods: the abduction brace and the sling. By examining clinical outcomes, pain management, tendon healing, and patient safety, we aim to provide a comprehensive overview of the current evidence and clinical practices.
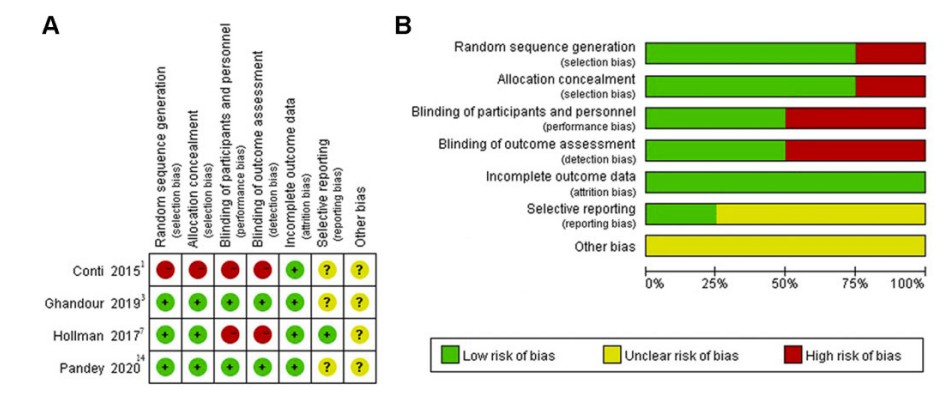 Fig.1 (A) Risk-of-bias summary for each included study and (B) each risk-of-bias item presented as a percentage across all included studies. (Gao J. H., et al., 2023)
Fig.1 (A) Risk-of-bias summary for each included study and (B) each risk-of-bias item presented as a percentage across all included studies. (Gao J. H., et al., 2023)
Clinical Outcomes: Constant-Murley Score

The Constant-Murley score (CMS) is a widely accepted metric for evaluating shoulder function postoperatively. It encompasses multiple dimensions, including pain, function, range of motion, and strength, providing a holistic assessment of the patient's recovery. A recent systematic review and meta-analysis compared the CMS values between patients using an abduction brace and those using a sling for postoperative immobilization. The results indicated no significant differences in CMS values at 3 months (WMD, 0.26 [95% CI, –1.30 to 1.83]; P = .74), 6 months (WMD, 1.91 [95% CI, –0.17 to 4.00]; P = .07), and 12 months (WMD, 0.55 [95% CI, –1.37 to 2.47]; P = .57) postoperatively. This suggests that both immobilization methods are equally effective in promoting shoulder function recovery. The absence of a significant difference in CMS values underscores the need for further investigation into the specific factors that may influence individual patient outcomes.
Pain Management: Visual Analog Scale Scores
Effective pain management is a cornerstone of postoperative care, particularly in procedures involving the rotator cuff. The visual analog scale (VAS) is a reliable tool for quantifying pain intensity, allowing for a standardized comparison across different immobilization methods. The meta-analysis revealed no significant differences in VAS pain scores between the abduction brace and sling groups at various time points: 1 week (WMD, 0.10 [95% CI, –0.20 to 0.41]; P = .51), 3 weeks (WMD, –0.12 [95% CI, –0.34 to 0.10]; P = .29), 6 weeks (WMD, –0.12 [95% CI, –0.30 to 0.06]; P = .20), and 12 weeks (WMD, –0.13 [95% CI, –0.27 to 0.02]; P = .09) postoperatively. This finding indicates that both immobilization methods provide comparable pain relief during the recovery period. The consistent pain management outcomes highlight the importance of personalized pain management strategies, as individual patient experiences may vary despite the overall statistical equivalence.
Tendon Healing: Retear Rates
One of the primary concerns following rotator cuff repair is the risk of retear, which can significantly impact long-term functional outcomes. The study pooled data from two RCTs to compare retear rates between the abduction brace and sling groups. The results showed no significant difference in retear rates at 3 months postoperatively (RR, 0.63 [95% CI, 0.09 to 4.23]; P = .64). This suggests that neither immobilization method offers a clear advantage in terms of tendon healing and retear prevention. The lack of a significant difference in retear rates underscores the complexity of tendon healing, which may be influenced by factors beyond immobilization, such as surgical technique, patient compliance, and individual biological factors.
Rehabilitation Protocols and Early Motion
Rehabilitation protocols play a crucial role in optimizing postoperative outcomes. An increasing number of physicians advocate for early motion protocols to enhance range of motion (ROM), alleviate pain, and facilitate an earlier return to activities. The study found no significant differences in ROM between the abduction brace and sling groups, suggesting that early motion protocols may be equally effective regardless of the immobilization method used. This finding supports the notion that early mobilization can be beneficial in promoting recovery without compromising tendon healing. However, the specific timing and extent of early motion should be tailored to individual patient needs and surgical findings.
Potential Complications and Patient Safety
While clinical outcomes and pain management are critical, patient safety must also be a priority. One study reported that using an abduction brace after rotator cuff repair is associated with a higher risk of falls due to visual field loss and body imbalance. This highlights the importance of considering patient safety when selecting an immobilization method. The potential for increased fall risk with abduction braces underscores the need for careful patient education and monitoring, especially during the early postoperative period. Future research should further explore the safety profiles of different immobilization methods to inform clinical decision-making.
Strengths and Limitations of the Study
The systematic review and meta-analysis offer valuable insights into the comparative effectiveness of abduction brace and sling immobilization. The study's strengths include its systematic approach and the inclusion of only randomized controlled trials (RCTs), which enhance the quality of evidence. However, limitations such as the small number of studies and patients included, the heterogeneity of clinical outcome measurements, and the short follow-up period for retear rate comparisons suggest that further research is needed to confirm these findings. Future studies should aim to address these limitations by incorporating larger cohorts, standardized outcome measures, and longer follow-up periods.
Conclusion
The systematic review and meta-analysis demonstrate that there are no significant differences between abduction brace and sling immobilization groups in terms of postoperative clinical scores, pain severity, and tendon healing. This suggests that abduction brace immobilization may not be necessary after arthroscopic rotator cuff repair. However, patient safety and individual needs should be carefully considered when selecting an immobilization method. Future research should focus on larger cohorts and longer follow-up periods to provide more definitive answers. The choice between an abduction brace and a sling for postoperative shoulder immobilization should be guided by a comprehensive assessment of patient-specific factors and clinical judgment.
Future Directions
Future studies should aim to address the limitations identified in this review. A larger number of high-quality RCTs with standardized outcome measures and longer follow-up periods are needed to provide more robust evidence. Additionally, further investigation into the potential complications associated with each immobilization method, such as the risk of falls with abduction braces, is warranted. By addressing these gaps, future research can contribute to a more nuanced understanding of the optimal postoperative care for patients undergoing rotator cuff repair.
If you have related needs, please feel free to contact us for more information or product support.
Reference
- Gao, Jing-Hui, et al. "Sling versus abduction brace shoulder immobilization after arthroscopic rotator cuff repair: a systematic review and meta-analysis." Orthopaedic Journal of Sports Medicine 11.8 (2023): 23259671231185368.
This article is for research use only. Do not use in any diagnostic or therapeutic application.
