If you are interested in products and services related to the research phase in this field, please contact for further inquiries.
Scaphoid fractures represent a significant challenge in orthopedic surgery, particularly when they result in nonunion. The scaphoid bone, located in the wrist, is crucial for wrist stability and function. Due to its unique anatomy and blood supply, scaphoid fractures are prone to complications such as nonunion, avascular necrosis, and humpback deformity. Traditional treatments, including headless compression screw fixation and bone grafting, have shown varying degrees of success. However, recent advancements in surgical techniques, particularly volar plate fixation, offer new hope for patients suffering from scaphoid fracture nonunion.
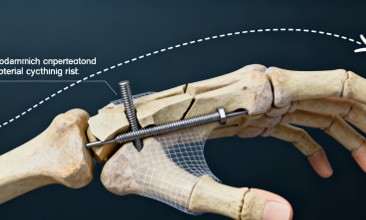
 Fig.1 Pre-operative radiographs (above) and computed tomographic scans (below) showing scaphoid waist nonunion, with approximately 10 mm of cystic erosion and bone loss at the nonunion site, with humpback deformity of the scaphoid and an early dorsal intercalated segment instability deformity of the wrist. (Dodds S. D., et al., 2018)
Fig.1 Pre-operative radiographs (above) and computed tomographic scans (below) showing scaphoid waist nonunion, with approximately 10 mm of cystic erosion and bone loss at the nonunion site, with humpback deformity of the scaphoid and an early dorsal intercalated segment instability deformity of the wrist. (Dodds S. D., et al., 2018)
Anatomical and Physiological Challenges of Scaphoid Fractures
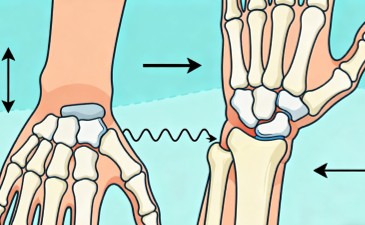
The scaphoid bone is an intra-articular bone, with nearly 80% of its surface covered by articular cartilage. This unique anatomy presents several challenges for healing:
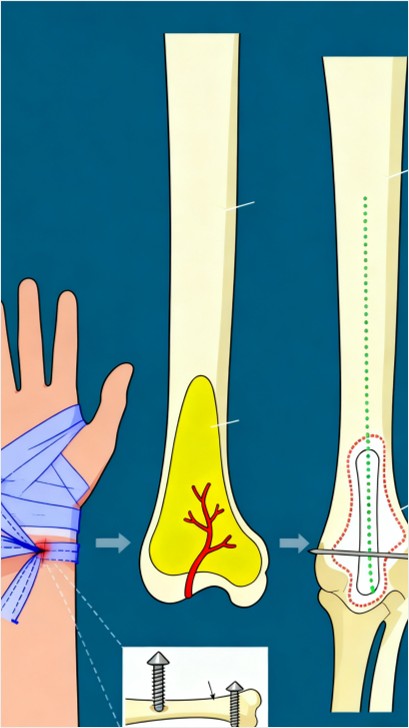
- Blood Supply: The scaphoid receives its blood supply primarily from a retrograde dorsal capsular artery, which often gets disrupted in fractures, leading to avascular necrosis of the proximal pole.
- Synovial Fluid: The presence of synovial fluid around the scaphoid can inhibit primary bone healing.
- Lack of Soft Tissue Attachments: The scaphoid has few soft tissue attachments, resulting in poor vascularity and inherent instability of fracture fragments.
- Intercalary Location: Situated between the proximal and distal carpal rows, the scaphoid experiences passive motion with every wrist movement, further complicating healing.
These factors contribute to a higher rate of nonunion in scaphoid fractures, particularly in cases with significant bone loss, humpback deformity, or avascular necrosis.
Traditional Treatments and Their Limitations
Headless Compression Screw Fixation
Headless compression screws have been the gold standard for treating scaphoid nonunions. They provide structural support by compressing the fracture fragments and preventing bending at the fracture site. However, this method has limitations:
- Bone Loss: In cases with significant bone loss, screws may not provide adequate support.
- Deformity: Humpback deformity or significant angulation may not be corrected effectively with screws alone.
- Avascular Necrosis: Screws do not address the issue of avascular necrosis, which can lead to further complications.
Bone Grafting
Bone grafts, either autografts or allografts, are often used to fill gaps and promote healing. However, bone grafting alone may not be sufficient:
- Placement Accuracy: Precise placement of the graft is crucial, and improper placement can lead to failure.
- Donor Site Morbidity: Harvesting bone grafts from other sites can lead to complications at the donor site.
- Limited Support: Bone grafts provide limited structural support and may not stabilize the fracture adequately.
Salvage Operations
In severe cases, salvage operations such as proximal row carpectomy or total wrist fusion are performed to relieve pain. However, these procedures result in permanent changes in wrist function:
- Loss of Wrist Motion: Total wrist fusion eliminates wrist motion, significantly impacting the patient's quality of life.
- Long-term Complications: These procedures can lead to adjacent joint arthritis and other long-term complications.
Volar Plate Fixation: A New Approach
Surgical Technique
Volar plate fixation represents a significant advancement in the treatment of scaphoid nonunions. The technique involves the use of a specially designed plate that provides robust support to the scaphoid bone. Key features of the technique include:
- Anatomical Contouring: The plate is pre-contoured to fit the volar aspect of the scaphoid, providing optimal support without the need for extensive intraoperative contouring.
- Buttress Support: Unlike screws, the plate offers significant buttress support, which is crucial in cases with significant humpback deformity or bone loss.
- Variable Screw Trajectories: The plate allows for non-locking and locking screws, providing flexibility in screw placement and ensuring secure fixation.
Surgical Steps
The surgical approach for volar plate fixation involves a volar, flexor carpi radialis approach, similar to that used for distal radial fractures. Key steps include:
- Exposure and Debridement: The nonunion site is exposed through a volar incision, and the radioscaphocapitate ligament is released to allow for better visualization and plate placement.
- Bone Graft Harvesting: A pedicled vascularized bone graft is harvested from the distal radius, providing a source of viable bone for the repair.
- Plate Placement: The pre-contoured plate is positioned on the volar aspect of the scaphoid, ensuring proper alignment and support. K-wires may be used provisionally to maintain reduction before screw insertion.
- Fixation: Non-locking screws are typically used first to ensure the plate is flush to the bone, followed by locking screws if needed.
Postoperative Care
Postoperative care is crucial for successful healing. Patients are typically immobilized in a short arm splint for 2 weeks, followed by a short arm cast for an additional month. A removable brace is used until clinical and radiographic signs of healing are observed. Ultrasound bone stimulation is often used as part of the postoperative protocol to promote healing.
Clinical Outcomes and Evidence
Case Series and Union Rates
A recent study by Dodds et al. (2017) evaluated the use of volar plate fixation in 20 consecutive patients with scaphoid nonunions. The patients had significant bone loss, humpback deformity, and in some cases, avascular necrosis. The results were promising:
- Union Rates: Clinical and radiographic evidence of union was observed in 18 out of 20 patients. Thirteen patients had CT scans showing at least 50% bridging bone, while the remaining five showed clinical evidence of union.
- Range of Motion: Postoperative range of motion improved in all patients, with mean flexion increasing from 52° to 58° and extension from 51° to 62°.
- Grip Strength: Grip strength also improved, with the treated wrist showing a mean grip strength of 39 kg compared to 32 kg preoperatively.
- Complications: There was one major complication (persistent nonunion) requiring revision and one minor complication (hematoma). Four patients experienced intermittent clicking with wrist flexion due to plate impingement, necessitating plate removal.
Comparative Analysis
Compared to traditional methods, volar plate fixation offers several advantages:
- Higher Union Rates: The high union rate observed in the study suggests that volar plate fixation is more effective in promoting healing.
- Improved Functional Outcomes: The significant improvement in range of motion and grip strength indicates better functional recovery.
- Reduced Complications: The use of a pedicled vascularized bone graft and pre-contoured plate reduces the risk of donor site morbidity and improper graft placement.
Future Directions and Research
Prospective Studies
Future research should focus on larger, prospective studies to validate the findings of this initial case series. Comparative studies with traditional methods, such as headless compression screw fixation, would provide valuable insights into the relative benefits and risks of each approach.
Long-term Follow-up
Long-term follow-up studies are needed to assess the durability of the results and the impact on patient quality of life. These studies should evaluate the long-term functional outcomes, including wrist motion, grip strength, and patient-reported outcomes.
Technological Advancements
Advancements in plate design and materials, as well as the development of new imaging techniques, can further enhance the efficacy of volar plate fixation. The integration of 3D printing and personalized plate design may offer even better outcomes in the future.
Conclusion
Volar plate fixation represents a significant advancement in the treatment of scaphoid fracture nonunions. By providing robust support and allowing for precise bone graft placement, this technique offers a promising alternative to traditional methods. While further research is needed to fully understand its long-term efficacy and potential complications, the initial results are encouraging. For patients facing the challenges of scaphoid nonunion, volar plate fixation may offer a new path to recovery and improved wrist function.
If you have related needs, please feel free to contact us for more information or product support.
Reference
- Dodds, Seth D., et al. "Lessons learned from volar plate fixation of scaphoid fracture nonunions." Journal of Hand Surgery (European Volume) 43.1 (2018): 57-65.
This article is for research use only. Do not use in any diagnostic or therapeutic application.